At the last full council meeting, Westminster City Council passed a motion on Health Inequalities by the Labour Group which was amended by the Tory Group whereby the council resolves to review any recommendations of PHE Report on COVID19 & Ethnic Minorities, incorporating them into the Council’s recovery strategy. These are top five recommendations l would make to reduce the impact of COVID19 to Westminsters ethnic minority communities within their corporate strategies.
- Work with Black & Asian Minority Ethnic communities in the City particularly their voluntary sector
BAME individuals are more likely to suffer from comorbidities, such as obesity or diabetes, and other health issues such as Vitamin D deficiency. The council should ensure that standard messaging on these public health issues is reinforced within BAME communities during the pandemic.
The council should also ensure that all public health information is provided in a wide range of languages including, but not limited to, Polish, Punjabi, Bengali, Arabic, Urdu, and Gujarati, French, Chinese, Portuguese and Spanish. At present, not all materials appear to be available in all of these languages.
And in this respect the council should work with the voluntary sector rooted in these communities like the Marylebone Bangladesh Society & Queens Park Bangladesh Association within the Bangladeshi community
- Protect and defend the Chinese community against racists accusations
From early in the pandemic, racist behaviour was observed against those of East Asian heritage due to the Chinese origin of the coronavirus. The council should remain vigilant against such behaviour and work with the Chinese community in the West End to support them against any potential resurgences For example, those arising from the publication of reports into the origins of the virus and every time Trump makes an anti-Chinese utterance!
- Better support for and understanding of intergenerational households
Much of the communication of guidance on household activities, including isolation and shielding, is mostly presented in the context of ‘traditional’ households. It should be recognised that intergenerational households are more common in Asian & Arab communities than White ones; and that these communities often contain a higher proportion of frontline healthcare workers. When older family members are co-resident with these workers, the risks of infection to those who are in a shielding group are elevated. Although some guidance on multi-generational households does exist, the council should undertake urgent consultations with members of these groups to explore how to better support them within the existing familial structures, and also to better understand the transmission of COVID-19 in such settings.
- Prioritisation of BAME individuals in Pillar 1 testing
The current testing prioritisation strategy used by the NHS does not make any mention of the increased risk to BAME individuals. The council should make the case to consider explicitly making ethnicity a factor in devising testing priority and frequency plans, both in Pillar 1 (“those with a medical need and the most critical key workers”) and the later pillars.
- Shielding
For individuals in a ‘moderate risk’ shielding group, consideration should be made of whether being from an ethnic minority is enough to justify moving the individual to the ‘high risk’ group in marginal cases. The extra concerns associated with shielding status must be allayed and should be considered within a socioeconomic context, such as the difficulty of isolation within a multigenerational household that includes frontline workers.
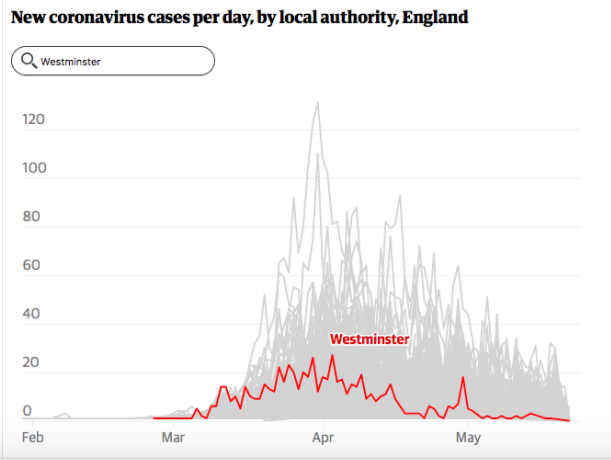
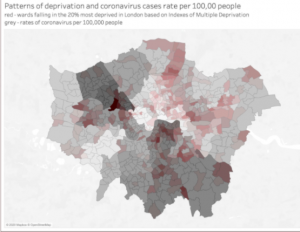
The five recommendations aside, it is clear that structural factors, such as discrimination in healthcare and education, play a substantial role, and manifest in a variety of different ways. These range from poorer healthcare literacy, to greater prevalence of underlying respiratory conditions from exposure to air pollution, to reduced access to public services. And in this respect residents of Westminster City Council are doing better than others in the overall picture in England and London as well, by measures of COVID19 daily cases; the actual number of fatalities and the patterns of deprivation and COVID19 cases per 100,000 people.
That said there are variations within the City of Westminster, like that between Church Street and St James & Mayfair localities which the council should be mindful when directing public health resources. For example in the former, we have had 21 fatalities so far while the latter has had only 2 going by the figures up to 31st of May.

This all comes at a time when Westminster City Council has been highlighted in a report to have only 13 per cent of its councillors from BAME communities even though its population is made up of 38 per cent of BAME communities. The Report suggested that the lack of BAME councillors ‘perpetuating racial inequality and disadvantage’ in the UK and something the Council needs to address urgently as well. A much more diverse Westminster City Council would no doubt have made the same recommendations to limit impact of COVID19.